All published articles of this journal are available on ScienceDirect.

PRK vs. LASIK in High Myopia: A Systematic Review and Meta-Analysis
Authors Info & Affiliations
Abstract
Introduction
To compare the efficacy, refractive predictability, and safety of photorefractive keratectomy (PRK) versus laser-assisted in situ keratomileusis (LASIK) in the treatment of high myopia. Unlike prior meta-analyses that evaluated mixed degrees of myopia, this study specifically focuses on high myopia (≥ –6.00 D) and incorporates more contemporary surgical techniques, providing a targeted assessment of outcomes in this higher-risk refractive population.
Methods
A systematic review and meta-analysis were performed according to PRISMA guidelines (PROSPERO CRD420251004602). PubMed, Web of Science, and Google Scholar were searched through March 2025 for randomized controlled trials and comparative studies that included patients with myopia ≥ −6.00 D and ≥9 months of follow-up. Outcomes included postoperative Spherical Equivalent (SE), uncorrected distance visual acuity (UDVA), refractive predictability (±0.50 D and ±1.00 D), and complications. Data were synthesized using random-effects models in RevMan 5.4.
Results
Eleven studies (n = 1,045 eyes) were included. Baseline SE was comparable between groups. At 1 and 12 months, no significant difference in SE was found, though PRK showed a better result at 6 months (MD = –0.29 D; P = 0.0003). Final UDVA (logMAR) did not differ (MD = 0.00; P = 0.95). LASIK achieved higher predictability, with significantly more eyes within ±0.50 D and ±1.00 D after excluding outliers. No difference was observed in the proportion of eyes reaching 20/20 vision, but LASIK was more likely to achieve 20/40 or better UDVA (OR = 0.52; P = 0.009). Complications varied: PRK was more frequently associated with corneal haze, particularly in studies that did not use intraoperative mitomycin-C (7/11 studies), whereas LASIK was more frequently associated with flap-related events.
Discussion
In eyes with high myopia, both PRK and LASIK demonstrated acceptable visual and refractive outcomes. Sensitivity analyses revealed that LASIK achieved superior refractive predictability within ±0.50 D and ±1.00 D, while final uncorrected visual acuity was comparable between procedures. PRK showed comparable refractive stability and remains a suitable option when corneal thickness or topography limits flap-based surgery. Compared with earlier systematic reviews, this analysis focuses specifically on high myopia and incorporates more contemporary evidence, reflecting modern refractive surgical practice. These findings support individualized procedure selection based on corneal characteristics and refractive goals.
Conclusion
PRK and LASIK provide comparable long-term efficacy in high myopia. LASIK offers superior refractive predictability and earlier functional vision, whereas PRK remains valuable in eyes unsuitable for LASIK, with haze risk largely mitigated by mitomycin-C.
1. INTRODUCTION
High myopia, defined as a refractive error of –6.00 diopters (D) or greater, is a major global public health concern due to its increasing prevalence and association with sight-threatening ocular complications such as retinal detachment, glaucoma, and myopic maculopathy [1, 2]. The worldwide prevalence of myopia has dramatically increased over the past few decades. As of 2020, approximately 30% of the global population was affected by myopia, and projections suggest that by 2050, nearly 50% of the global population will be myopic, with 10% of those developing high myopia, amounting to approximately 1 billion people [3]. Laser corneal refractive surgery has become a highly effective and predictable method for correcting myopia and reducing dependence on spectacles and contact lenses [4, 5]. PRK is considered a safe and effective option for vision correction. However, it has certain limitations, including delayed epithelial healing, postoperative pain, stromal haze, and the risk of corneal ectasia. [6-8]. With the introduction of LASIK, many surgeons prefer it as the primary choice due to its faster visual recovery and reduced discomfort in the early postoperative period. [9]. Nevertheless, PRK remains the preferred surgical option for patients with irregular corneal topography, thinner corneas, or those who do not qualify for LASIK [8].
Despite extensive evidence comparing PRK and LASIK in mild and moderate myopia, data in high myopia remain limited. The only prior systematic review addressing this topic found comparable long-term visual and refractive outcomes between the two procedures [10]. Previous systematic reviews comparing PRK and LASIK have largely evaluated mixed degrees of myopia and did not isolate high myopia (≥ –6.00 D) as a primary analytic population. The presents analysis incorporates newer studies reflecting the widespread adoption of femtosecond flap creation in LASIK, optimized excimer laser ablation profiles, and routine intraoperative mitomycin-C use in PRK. These technological advancements have significantly influenced refractive predictability, wound healing response, and complication profiles, particularly in highly myopic eyes. Given the distinct biomechanical and refractive challenges posed by high myopia compared with low to moderate myopia, a focused evaluation of this subgroup using more contemporary evidence is clinically warranted. To our knowledge, a dedicated meta-analysis specifically targeting high myopia in the modern surgical era has not been previously performed. This systematic review and meta-analysis, therefore, aimed to comprehensively compare the efficacy, safety, and long-term outcomes of PRK and LASIK in patients with high myopia to inform current surgical decision-making and patient selection.
2. METHODS AND MATERIALS
2.1. Study Registration
This systematic review was conducted according to a predefined protocol, registered with PROSPERO (CRD420251004602). The reporting of this review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [11].
2.2. Search Strategy
Two reviewers independently searched the electronic databases PubMed, Web of Science, and Google Scholar through March 2025 to identify relevant studies comparing photorefractive keratectomy (PRK) and laser-assisted in situ keratomileusis (LASIK) for the treatment of high myopia. Search terms included combinations of “LASIK,” “photorefractive keratectomy,” “PRK,” “high myopia,” “refractive surgery,” and “severe myopia.” Titles and abstracts were initially screened for relevance. Full-text articles were then reviewed for eligibility based on predefined inclusion criteria. Additional manual searches of the reference lists of included articles were conducted to identify additional relevant studies. Any disagreements regarding study selection were resolved by a third reviewer through discussion and consensus.
2.3. Eligibility Criteria
In this review, we included studies that compared patients who underwent PRK or LASIK for the treatment of high myopia, with or without associated myopic astigmatism. We excluded studies involving patients with prior refractive or intraocular surgery, as well as those with ocular comorbidities or systemic conditions known to affect corneal healing or visual outcomes. We included both Randomized Controlled Trials (RCTs) and non-randomized comparative studies with a follow-up duration of at least 9 months, provided they reported on one or more of the prespecified outcomes, such as spherical equivalent stability, refractive predictability, or visual acuity.
2.4. Definition of High Myopia and Handling of Surgical Technique Variability
High myopia was defined as a preoperative spherical equivalent of −6.00 diopters or greater. Studies including mixed refractive ranges were included only if data for eyes meeting this threshold could be extracted separately.
With respect to surgical technique heterogeneity, variations within each treatment group were anticipated, given the long study period and evolution of refractive surgery techniques. The PRK group included conventional PRK, transepithelial PRK, and advanced surface laser ablation, as these procedures share a common surface ablation principle without flap creation. The use of MMC was recorded when reported. However, due to inconsistent reporting and limited sample sizes, studies were not stratified by MMC use for quantitative meta-analysis. Similarly, the LASIK group included femtosecond laser-assisted LASIK and microkeratome LASIK, both of which involve lamellar flap creation followed by excimer laser ablation.
Given the limited number of studies and heterogeneous reporting of surgical subtypes, all PRK and LASIK techniques were analyzed within their respective categories to preserve statistical power and reflect real-world clinical practice. The potential impact of this within-group heterogeneity was explored qualitatively and is addressed in the Discussion as a limitation of the current analysis.
2.5. Quality Assessment of Retrieved Articles
Two reviewers independently assessed the risk of bias for all included studies. For RCTs, we used the Cochrane Risk of Bias 2.0 (RoB 2) tool, which evaluates five domains: randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selection of the reported result. Studies were classified as having low risk, some concerns, or high risk of bias [12]. For non-randomized comparative studies, we applied the ROBINS-I (Risk of Bias in Non-randomized Studies - of Interventions) tool. This tool assesses seven domains: confounding, participant selection, classification of interventions, deviations from intended interventions, missing data, measurement of outcomes, and selection of the reported result. Studies were rated as having low risk, moderate risk, serious risk, critical risk, or no information [13]. Any discrepancies in risk-of-bias judgments were resolved through discussion and consensus among the reviewers.
2.6. Outcome Measures
The primary outcome measures of this meta-analysis were designed to assess the efficacy and refractive predictability of PRK and LASIK in the treatment of high myopia. These included the final mean Spherical Equivalent (SE) at the last reported follow-up, the proportion of eyes achieving an Uncorrected Distance Visual Acuity (UDVA) of 20/20 or better, the proportion achieving UDVA of 20/40 or better, and the proportion of eyes within ±0.50 diopters and ±1.00 diopters of the intended target refraction. In addition, commonly reported postoperative complications were noted. However, due to inconsistent definitions and reporting formats across studies, complications were summarized descriptively rather than being included in the quantitative meta-analysis.
2.7. Meta-analysis
The meta-analysis was conducted using Review Manager (RevMan) version 5.4 (Cochrane Collaboration). For all outcomes, we applied the inverse-variance method, using the mean difference (MD) for continuous outcomes and the Mantel-Haenszel method with odds ratios (ORs) for dichotomous outcomes. This study used the random-effects model for all meta-analyses due to expected clinical and methodological heterogeneity across studies. Statistical significance was set at a 95% confidence level, with p < 0.05 considered statistically significant. Continuous outcomes included preoperative and postoperative spherical equivalents at 1, 6, and 12 months, all analyzed using Mean Difference (MD). Dichotomous outcomes included the proportions of eyes achieving UDVA of 20/20 or better and 20/40 or better, and the proportions of eyes within ±0.50 D and ±1.00 D of target refraction. A sensitivity analysis was conducted for outcomes with substantial heterogeneity by excluding the study or studies that contributed most to the inconsistency to assess the stability of the pooled estimates.
3. RESULTS
3.1. Study Selection
The study selection process is illustrated in Fig. (1). The initial search identified 385 records. After excluding 56 duplicates, 329 titles and abstracts underwent screening. Subsequently, 23 full-text articles were evaluated for eligibility, and 11 studies were ultimately included in the review. The baseline characteristics of these 11 studies are summarized in Table 1.
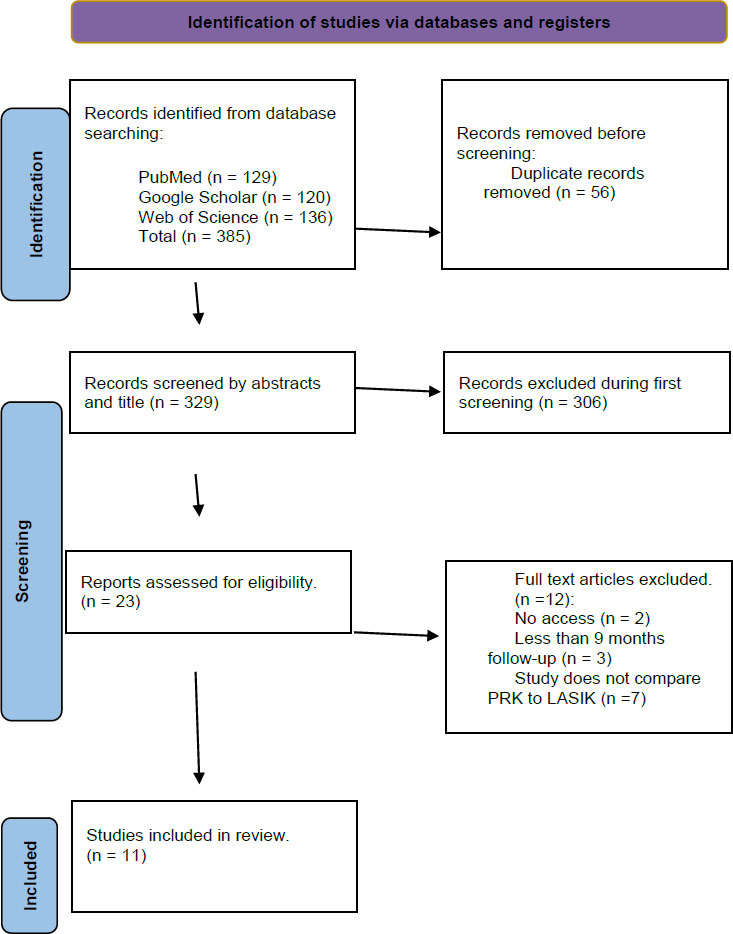
Flowchart illustrating the study selection process for the systematic review and meta-analysis comparing PRK and LASIK in the treatment of high myopia.
Summary of study design, sample size, age, preoperative spherical equivalent (SE), and preoperative uncorrected distance visual acuity (UDVA) for both PRK and LASIK groups across the 11 included studies.
| Study | Study Design | Total Number of Patients (number of eyes) | Total Number of PRK Patients (number of eyes) | Total Number of LASIK Patients (number of eyes) | Age in Years (mean ± SD) | PRK Group Degree of Myopia (mean ± SD in diopters, preoperative) | LASIK Group Degree of Myopia (mean ± SD in diopters, preoperative) | PRK Group UDVA (mean ± SD, logMAR or Snellen) | LASIK Group UDVA (mean ± SD, logMAR or Snellen) |
|---|---|---|---|---|---|---|---|---|---|
| Zhang, Y et al. 2022 [16] | Prospective interventional study | 32 patients, 64 eyes | 32 eyes | 32 eyes | 18 years or older | −6.57 ± 2.01 D | −6.67 ± 1.99 D | 1.07 ± 0.22 logMAR | 1.08 ± 0.23 logMAR |
| Mounir et al. 2020 [14] | Prospective comparative interventional study | 156 patients,156 eyes | 72 eyes | 84 eyes | PRK group: 29.76±5.01 LASIK group: 27.94±6.69 |
-8.86±1.81 D | -9.25±1.70 D | 0.05±0.02 | 0.05±0.01 |
| Jiafan Zhang et al. 2020 [17] | Prospective, non-randomized, cohort study | 88 patients, 165 eyes | 46 patients, 85 eyes | 80 eyes of 42 patients | PRK group: 25.6 ± 6.1, LASIK group: 23.9 ± 5.5 |
−7.59 ± 0.84 D | −7.60 ± 1.21 D | 1.22 ± 0.20 logMAR | 1.25 ± 0.21 logMAR |
| Hashemi 2016 et al. [15] | Comparative nonrandomized clinical trial | 30 patients, 60 eyes | 30 eyes | 30 eyes | PRK group: 27.14 ± 5.63 LASIK group: 28.60 ± 7.85 |
-8.54 ± 1.42 D | -8.19 ± 2.05 D | 1.75 ± 0.16 logMAR | 1.80 ± 0.15 logMAR |
| Ioannis M Aslanides, 2014 et al. [18] | Prospective interventional cohort with matched retrospective control groups | 64 patients, 101 eyes | tPRK group: 27 patients (41 eyes) standard PRK group: 20 patients (29 eyes) | 17 patients, 31 eyes | tPRK: 27 ± 6 PRK: 27 ± 6 LASIK: 31.3 ± 10 | tPRK: -7.89 ± 1.24D PRK: -8.25 ± 1.72 D |
-7.41 ± 1.35 D | N/A | N/A |
| Anders Ivarsen et al. 2009 [37] | Randomized clinical trial | 46 patients, 46 eyes | 20 patients, 20 eyes | 25 patients, 25 eyes | PRK: 33± 8 LASIK:30± 7 | -6.91 ± 0.57 D | -7.12 ± 0.57 D | N/A | N/A |
| Jorge L. Alió et al. 2009 [20] | Retrospective study | 192 eyes | 51 eyes | 141 eyes | PRK: 33.96 ± 10.96 (20 to 66) LASIK: 32.44 ± 9.09 |
–12.44 ± 1.49 D | –12.81±1.64 D | N/A | N/A |
| Jorge L. Alió et al. 2010 [21] | Retrospective, control-matched study | 65 patients, 68 eyes | 33 patients, 34 eyes | 32 patients, 34 eyes | PRK: 29.4 (6.8), LASIK 29.44 (6.8) | –8.42 ± 1.34 D | –8.30± 1.21 D | N/A | N/A |
| Hjortdal et al. 2005 [22] | Prospective randomized study | 45 patients, 45 eyes | 20 patients, 20 eyes | 25 patients, 25 eyes | PRK (n=20) 33± 8, LASIK (n=25) 30± 7 | –6.64 ± 0.55 D | -7.12 ± 0.57 D | N/A | N/A |
| Langrová et al. 2003 [23] | Comparative study | 89 patients, 89 eyes | 38 patients, 38 eyes | 31 patients, 31 eyes | PRK: mean age of 25 (18± 48), LASIK: mean age of 24 years (19± 48) |
–-8.0± 1.7 D | -9.2± 2.1 D | N/A | N/A |
| A. Helmy et al. 1996 [24] | Randomized clinical trial | 59 patients, 80 eyes | 40 eyes | 40 eyes | Mean: 29 | -7 D | -7.3 D | N/A | N/A |
Quality assessment of the included studies is shown in Figs. (2 and 3). All non-randomized studies showed a moderate risk of bias, mainly due to confounding and deviations from interventions (Fig. 2). In contrast, RCTs showed a low risk of bias, with concerns noted in one study [14] regarding randomization and missing outcome data (Fig. 3).
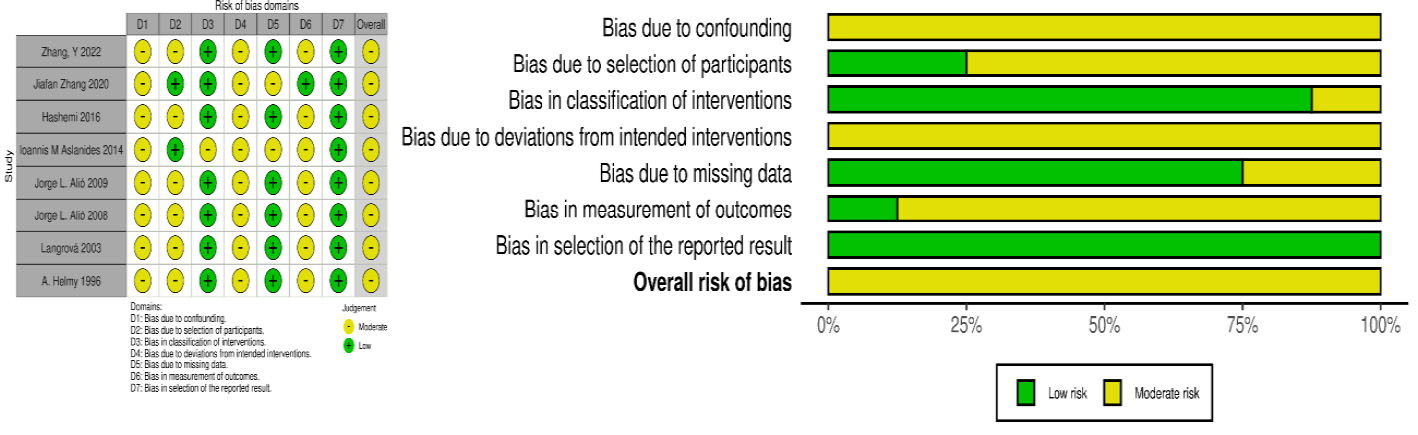
Risk of bias summary for non-randomized studies assessed using the ROBINS-I tool, showing low risk (green) and moderate risk (yellow) across seven domains.
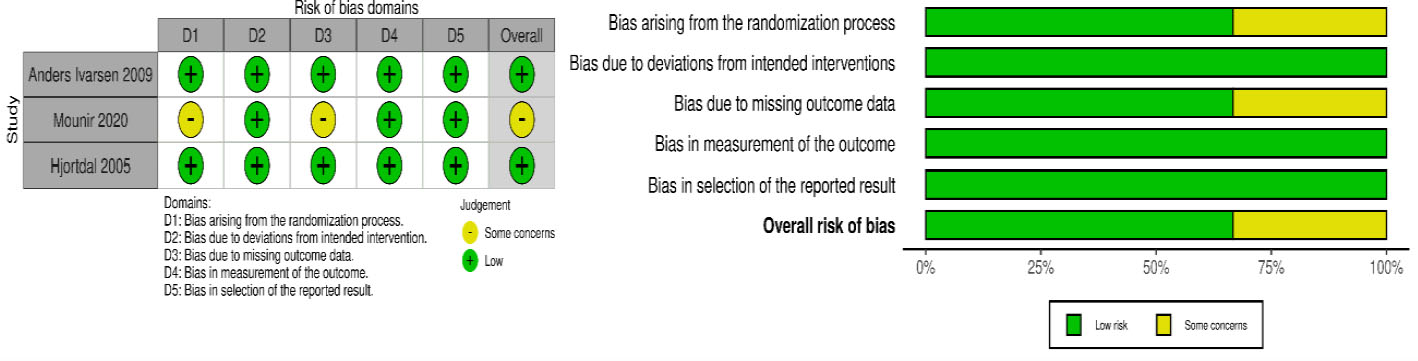
Risk of bias summary for randomized controlled trials assessed using the RoB 2.0 tool, showing low risk (green) and some concerns (yellow) across five domains.
Baseline SE was compared as shown in Fig. (4) across ten studies [14-23]. The pooled analysis revealed a comparable baseline SE between PRK and LASIK groups (MD, 0.17 D; 95% Cl, -0.07 to 0.42; P = 0.16), with no statistical or clinical significance.
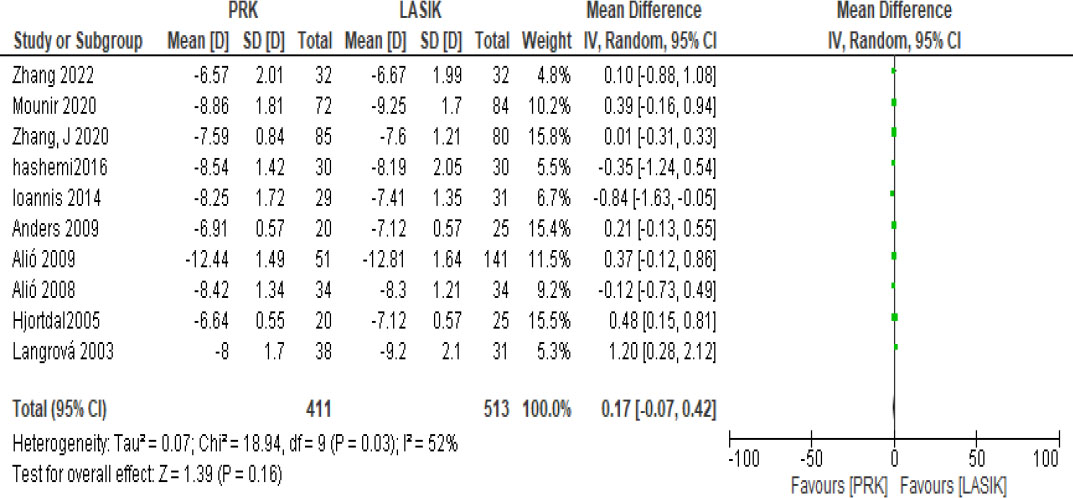
Comparison of baseline spherical equivalent (SE) between PRK and LASIK groups. The pooled mean difference was 0.17 D (95% CI: -0.07 to 0.42; p = 0.16), indicating no statistically or clinically significant difference.
Of the 11 studies, 4 studies reported SE at 1 month postoperatively, as shown in Fig. (5) [14, 16, 19, 22]. The initial analysis showed no statistically significant difference in refractive stability between PRK and LASIK (MD, 0.37 D; 95% CI, -0.26 to 0.99; P = 0.25). A sensitivity analysis excluding Hjortdal 2005, [22] markedly reduced heterogeneity from 94% to 56% and confirmed non-significance (MD, -0.04 D; 95% CI, -0.30 to 0.22; P = 0.77). The small numerical difference is not statistically or clinically meaningful.
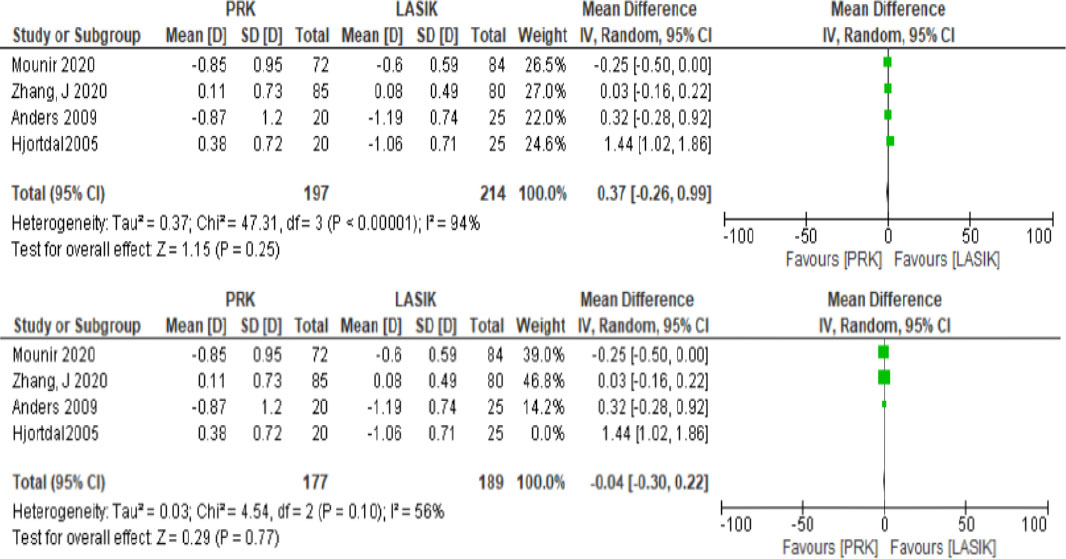
Spherical equivalent at 1 month postoperatively showed no statistically significant difference between PRK and LASIK (MD = 0.37 D; 95% CI: -0.26 to 0.99; p = 0.25; I2 = 94%). After excluding Hjortdal 2005, heterogeneity decreased to 56% and results remained non-significant (MD = -0.04 D; 95% CI: -0.30 to 0.22; p = 0.77), indicating improved consistency.
Five studies evaluated SE at 6 months postoperatively, as shown in Fig. (6) [14, 15, 17, 19, 22]. The overall pooled estimate showed no significant difference (MD, -0.16 D; 95% CI, -0.39 to 0.07; P = 0.18), with moderate heterogeneity (I2 = 68%). After excluding Zhang J 2020, [17] heterogeneity was eliminated (I2 = 0%), and the statistical result became significant (MD, -0.29 D; 95% CI, -0.45 to –0.14; P = 0.0003), favoring PRK over LASIK.
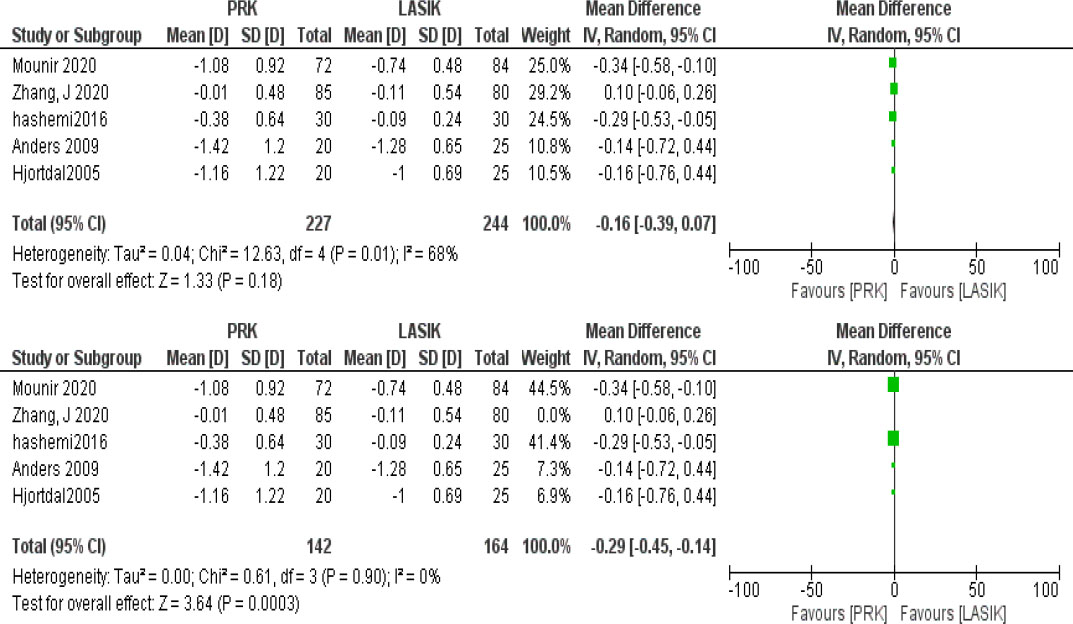
Forest plots comparing spherical equivalent at 6 months postoperatively between PRK and LASIK. In the initial analysis (top), there was no significant difference (MD = –0.16 D; 95% CI: –0.39 to 0.07; p = 0.18; I2 = 68%). After excluding Zhang J 2020 (bottom), the result became statistically significant in favor of PRK (MD = –0.29 D; 95% CI: –0.45 to –0.14; p = 0.0003) with no heterogeneity (I2 = 0%).
Nine studies reported data about SE at 12 months postoperatively as shown in Fig. (7) [14, 16-23]. Analysis of these data indicated no statistically significant difference between PRK and LASIK (MD, -0.03 D; 95% CI, -0.19 to 0.13; P = 0.67), with moderate heterogeneity (I2 = 69%). After excluding Alió 2009, [20] heterogeneity reduced to 50%, and the effect estimate remained non-significant (MD, 0.03 D; 95% CI, -0.09 to 0.16; P = 0.62).
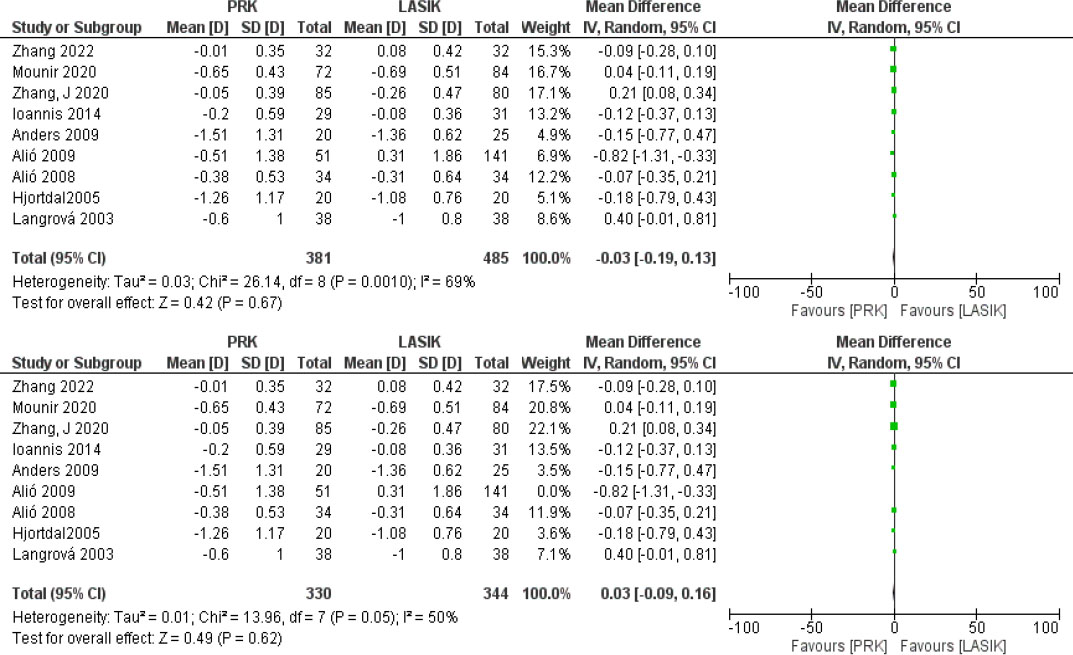
Forest plots comparing spherical equivalent at 1 year postoperatively between PRK and LASIK. In the full analysis including all studies (top), no statistically significant difference was observed (MD = –0.03 D; 95% CI: –0.19 to 0.13; p = 0.67; I2 = 69%). After excluding Alió 2009 (bottom), heterogeneity improved to 50%, and the result remained non-significant (MD = 0.03 D; 95% CI: –0.09 to 0.16; p = 0.62), confirming comparable refractive stability between the two procedures at 1 year.
UDVA logMAR at final follow-up was compared between PRK and LASIK across four studies, as shown in Fig. (8). The initial analysis showed no significant difference between the two groups (Mean Difference = 0.00; 95% CI: -0.03 to 0.03; P = 0.95), with substantial heterogeneity (I2 = 65%). After excluding the Hashemi 2016 study, the analysis included three studies, and the results remained non-significant (Mean Difference = -0.02; 95% CI: -0.04 to 0.00; P = 0.10), with heterogeneity reduced to 25%, indicating improved consistency. Overall, these findings suggest that both PRK and LASIK provide comparable uncorrected distance visual acuity outcomes at final follow-up.
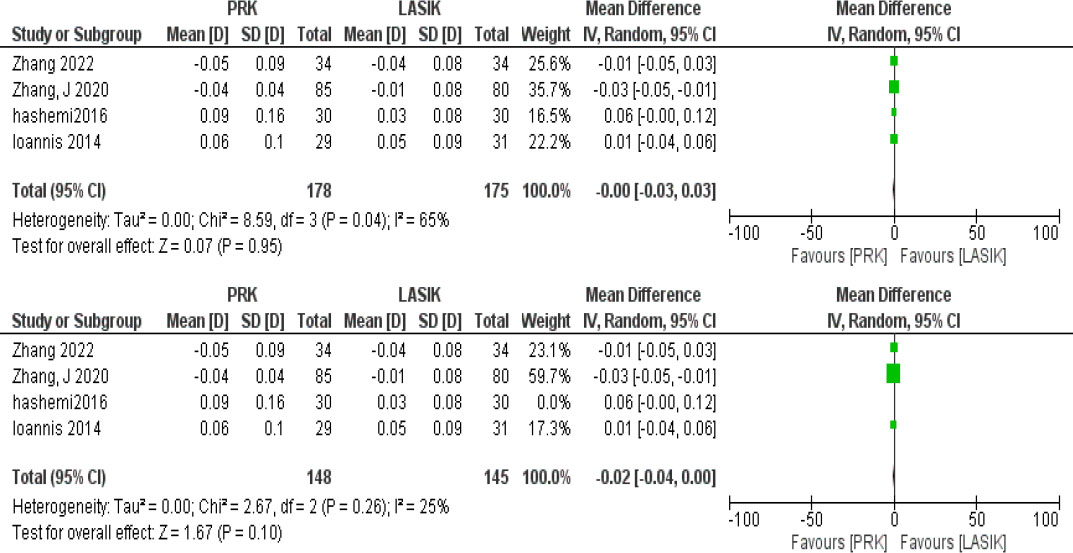
Forest plots comparing uncorrected distance visual acuity (UDVA, logMAR) at final follow-up between PRK and LASIK. The initial analysis, including all four studies (top), showed no significant difference (MD = –0.00; 95% CI: –0.03 to 0.03; p = 0.95) with moderate heterogeneity (I2 = 65%). After excluding Hashemi 2016 (bottom), the difference remained non-significant (MD = –0.02; 95% CI: –0.04 to 0.00; p = 0.10), and heterogeneity decreased to 25%, indicating improved consistency.
This figure compares PRK and LASIK in achieving a refractive outcome within ±0.50 diopters of the target, as shown in Fig. (9). The upper analysis, which includes all studies, shows no statistically significant difference between the two procedures (OR = 0.75, 95% CI: 0.36–1.54), and is marked by moderate heterogeneity (I2 = 69%). In contrast, the lower analysis excluding the Zhang J 2020 study demonstrates a statistically significant advantage for LASIK (OR = 0.54, 95% CI: 0.31–0.94), with substantially reduced heterogeneity (I2 = 33%). These findings indicate that LASIK is associated with more consistent and predictable refractive outcomes than PRK, with a greater proportion of eyes achieving close alignment with the intended correction.
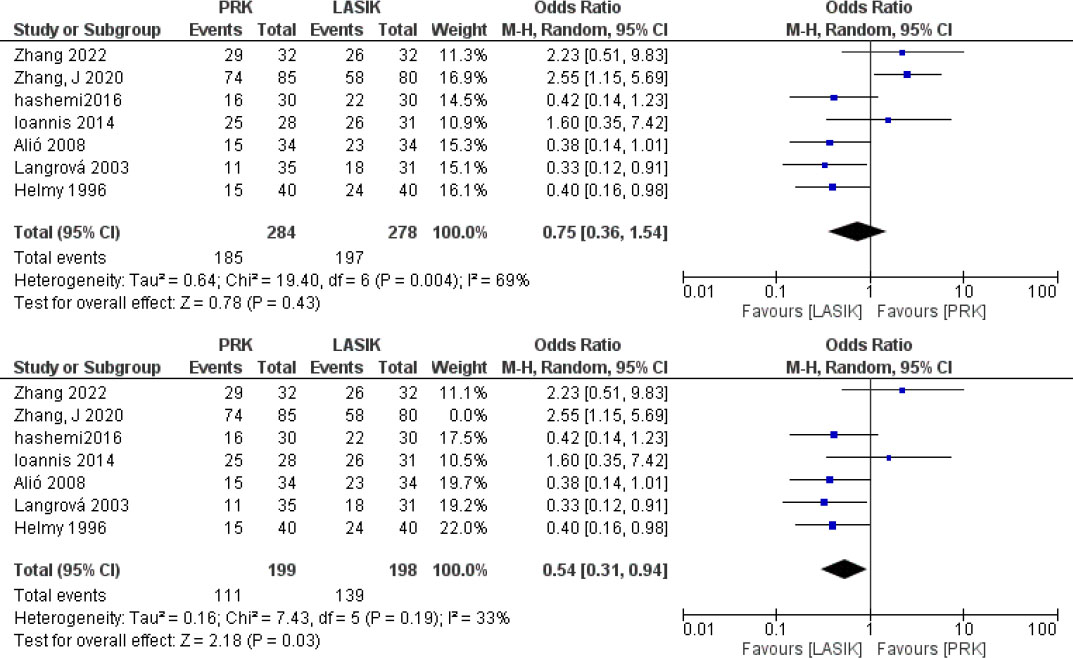
Forest plots comparing the proportion of eyes within ±0.50 D of target refraction between PRK and LASIK. The initial analysis (top) showed no significant difference (OR = 0.75; 95% CI: 0.36–1.54; I2 = 69%). After excluding Zhang J 2020 (bottom), LASIK showed significantly better refractive predictability (OR = 0.54; 95% CI: 0.31–0.94; p = 0.03), with reduced heterogeneity (I2 = 33%), enhancing confidence in the result.
The initial analysis of eight studies in Fig. (10) showed no statistically significant difference in achieving refractive outcomes within ±1.00 D between PRK and LASIK (OR = 0.72; 95% CI: 0.36–1.45; p = 0.36), with moderate heterogeneity (I2 = 63%). After excluding Zhang J 2020 and Hjortdal 2008, the results became statistically significant in favor of LASIK (OR = 0.52; 95% CI: 0.29–0.92; p = 0.03), with heterogeneity reduced to 47%. These findings suggest that LASIK provides better refractive predictability than PRK when outlier studies are removed.
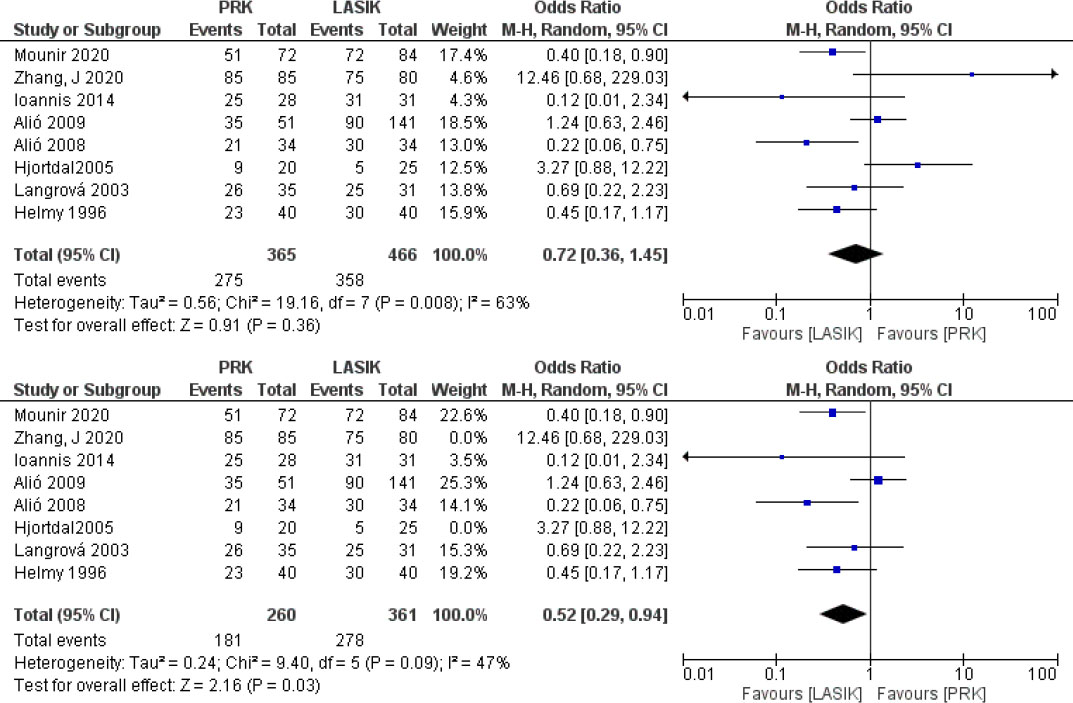
Forest plots comparing the proportion of eyes within ±1.00 D of target refraction between PRK and LASIK. The initial analysis (top) showed no significant difference (OR = 0.72; 95% CI: 0.36–1.45; I2 = 63%). After excluding Zhang J 2020 and Hjortdal 2005 (bottom), LASIK showed significantly higher odds of achieving refractive accuracy within ±1.00 D (OR = 0.52; 95% CI: 0.29–0.94; p = 0.03), with reduced heterogeneity (I2 = 47%). This supports better predictability for LASIK.
Data from six studies comparing the number of eyes achieving 20/20 vision or better following PRK versus LASIK are shown in Fig. (11). In the initial analysis, including all studies, no statistically significant difference is found between the two procedures (OR = 1.01, 95% CI: 0.48–2.15, p = 0.97), with moderate heterogeneity (I2 = 48%). After excluding Zhang J 2020, the odds ratio shifts in favor of PRK (OR = 0.81), although the result remains statistically non-significant (95% CI: 0.41–1.61, p = 0.55), and heterogeneity is further reduced to a low level (I2 = 30%). As the confidence intervals cross 1 in both analyses, no definitive advantage of PRK or LASIK can be concluded in achieving 20/20 or better vision, though the trend slightly favors PRK after excluding Zhang J 2020.
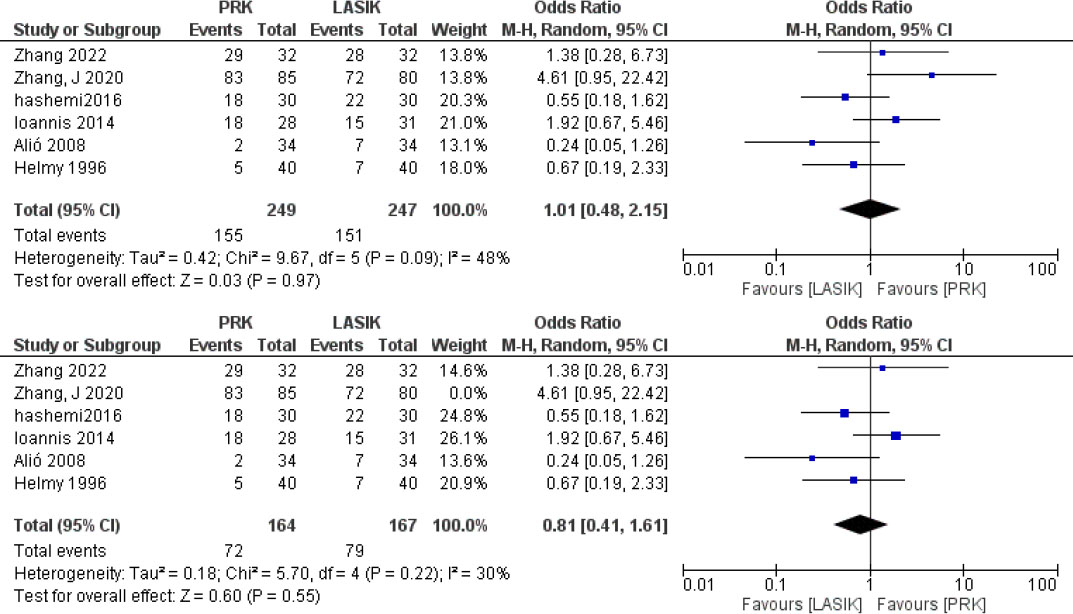
Forest plots comparing the proportion of eyes achieving UDVA of 20/20 or better after PRK versus LASIK. The initial analysis (top) showed no significant difference between the two groups (OR = 1.01; 95% CI: 0.48–2.15; p = 0.97; I2 = 48%). After excluding Zhang J 2020 (bottom), the result remained non-significant (OR = 0.81; 95% CI: 0.41–1.61; p = 0.55) with lower heterogeneity (I2 = 30%), increasing confidence in the finding of comparable visual outcomes.
A total of 5 studies reported the proportion of eyes achieving 20/40 or UDVA following PRK or LASIK, as shown in Fig. (12). The initial pooled analysis showed no statistically significant difference between the two procedures (OR = 0.64; 95% CI: 0.31–1.32; p = 0.23), with moderate heterogeneity (I2 = 42%). After removing the outlier study by Zhang J 2020, the analysis demonstrated a statistically significant advantage for LASIK (OR = 0.52; 95% CI: 0.32–0.85; p = 0.009), with no evidence of heterogeneity (I2 = 0%). These results indicate that LASIK is more likely to achieve 20/40 or better vision, with improved consistency across studies.
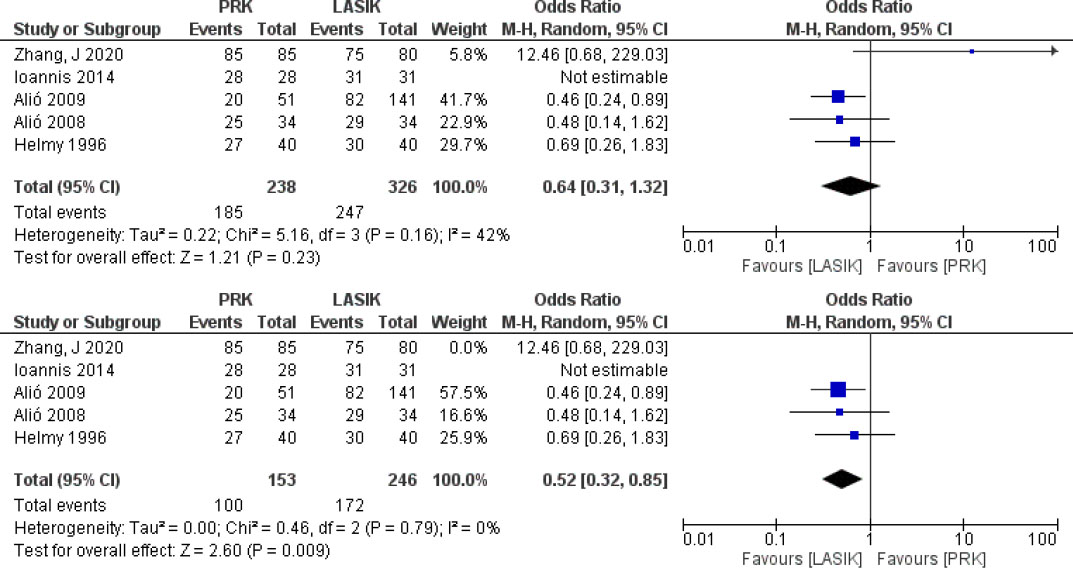
Forest plots comparing the proportion of eyes achieving UDVA of 20/40 or better after PRK versus LASIK. In the full analysis (top), no significant difference was observed (OR = 0.64; 95% CI: 0.31–1.32; p = 0.23; I2 = 42%). After excluding Zhang J 2020 (bottom), LASIK showed a statistically significant advantage (OR = 0.52; 95% CI: 0.32–0.85; p = 0.009), with no heterogeneity (I2 = 0%). These findings suggest LASIK is more likely to achieve 20/40 or better outcomes, with consistent results across studies.
Secondary outcomes reported by each study and categorized by procedure (PRK vs. LASIK) are summarized in Table 2. The table demonstrates variability in the type and frequency of postoperative complications across both procedures. Corneal haze was more commonly associated with PRK, as evidenced by reports in 8 studies [14, 16, 18, 19, 20, 21, 23, 24], in contrast to LASIK, where only 2 studies documented its occurrence [16, 25]. Moreover, both procedures showed distinct adverse events. LASIK has more flap-related complications, as indicated by findings from 3 studies [14, 20, 22]. In contrast, PRK was characterized by complications such as delayed epithelial healing and haze formation. Corneal haze was reported more frequently after PRK in 8 studies; however, it is important to note that most of these studies did not use intraoperative MMC, which is now routinely applied to reduce haze risk [14, 15, 16, 18].
| Study | Corneal Haze | Adverse Effects | ||
|---|---|---|---|---|
| PRK | LASIK | PRK | LASIK | |
| Zhang Y et al. 2022 [16] | -0.5 in 17 eyes -1.0 in 10 eyes |
- 0.5 in 19 eyes -1.0 in 4 eyes |
N/A | N/A |
| Mounir et al. 2020 [14] | 2 eyes: -Grade 2: 1 eye -Grade 4: 1 eye |
N/A | -Delayed epithelial healing in two eyes. -One eye suffered from toxic epitheliopathy. |
-Two eyes with released suction ring and two eyes with microstriae which were corrected by re-floating the flap. |
| Jiafan Zhang et al. 2020 [17] | N/A | N/A | N/A | N/A |
| Hashemi et al. 2016 [15] | N/A | N/A | N/A | N/A |
| Ioannis M Aslanides et al. 2014 [18] |
tPRK group: -3 months: 15 eyes -6 months: reduced to 9 eyes -12 months: 1 eye PRK group: -3 months: 6 eyes -6 months: 5 eyes -12 months: 0 eyes |
N/A | N/A | N/A |
| Anders Ivarsen et al. 2009 [37] | 1 eye | N/A | N/A | N/A |
| Jorge L. Alió et al. 2009 [20] | -Graded on a scale of 0 to 4 Grade 1: -18 eyes at 3 months -2 years: 18 eyes -10 years: 6 eyes |
N/A | - 6 eyes lost 2 or more lines of CDVA. - 4 eyes lost lines due to CNVM formation. - 2 eyes lost lines due to the presence of haze. |
- 7 eyes lost 2 or more lines of CDVA. - 2 eyes lost lines due to choroidal neovascular membrane formation. - 1 eye lost lines due to retinal detachment. - 4 eyes lost lines due to cataract formation. |
| Jorge L. Alió et al. 2010 [21] | At 10 years, one of 34 eyes had grade 0.5 haze | N/A | - Central island in 2 of 34 eyes; resolved spontaneously or corrected. | - Fine wrinkles (one of 34 eyes) confined to the flap and did not affect vision. - Corneal flap melt or necrosis (one of 34 eyes). |
| Hjortdal et al. 2005 [22] | N/A | N/A | -Peripheral flap edema and corneal epithelial thinning | -Peripheral flap edema and corneal epithelial thinning |
| Langrová et al. 2003 [23] | 4 patients | N/A | N/A | N/A |
| A. Helmy et al. 1996 [24] | Mean haze: -1 month: 1.70 ± 0.56 -3 months: 1.70 ± 0.67 -6 months: 1.60 ± 1.07 -12 months: 1.20 ± 0.42 |
Mean haze: -1 month: 1.37 ± 0.74 -3 months: 0.75 ± 0.74 -6 months: 0.50 ± 0.53 -12 months: 0.25 ± 0.46 |
N/A | N/A |
4. DISCUSSION
In this systematic review and meta-analysis, we compared the safety and efficacy of PRK and LASIK specifically in eyes with high myopia. While both procedures demonstrated acceptable visual and refractive outcomes, LASIK showed superior refractive predictability within ±0.50 D and ±1.00 D in sensitivity analyses with reduced heterogeneity. These findings suggest that, in appropriately selected high myopic eyes, LASIK may offer more consistent refractive accuracy, whereas PRK remains a viable alternative in cases where corneal thickness or topography preclude flap-based surgery. Importantly, differences between procedures were more apparent after accounting for influential studies, highlighting the impact of study design and patient selection on pooled outcomes.
The findings of this meta-analysis should be interpreted in the context of prior systematic reviews. Shortt et al. (2006) and the subsequent Cochrane update by Shortt et al. (2013) compared PRK and LASIK across a broad spectrum of myopia and concluded that LASIK offered faster visual recovery, with largely comparable long-term visual and refractive outcomes [10, 26]. However, those reviews primarily included studies conducted before widespread adoption of modern excimer platforms, femtosecond flap creation, routine MMC use in PRK, and contemporary ablation algorithms. In addition to isolating high myopia as the primary analytic population, this study contributes several additional findings not previously emphasized in earlier meta-analyses. These include a focused evaluation of refractive predictability within ±0.50 D and ±1.00 D in high myopic eyes, sensitivity analyses demonstrating the influence of specific outlier studies on heterogeneity, and an assessment of medium-term refractive stability at 6 months following exclusion of influential data. These analyses provide a more granular understanding of refractive outcomes in high myopia than previously reported.
Although newer refractive techniques such as small incision lenticule extraction (SMILE) have become increasingly popular for myopic correction, the clinical decision between surface ablation and lamellar procedures remains highly relevant, particularly in patients with high myopia or reduced corneal thickness. SMILE is generally limited by the lack of cyclotorsion control and is not suitable for cases requiring customized ablation profiles or topography-guided treatments [19, 27]. In contrast, PRK and LASIK remain the primary options for patients with thin or irregular corneas, previous ocular surgery, or borderline residual stromal bed thickness. Despite abundant comparative data on PRK and LASIK in low-to-moderate myopia, studies focused exclusively on high myopia are scarce. The present meta-analysis, therefore, provides an updated synthesis of modern refractive outcomes, incorporating recent evidence on the use of intraoperative MMC to mitigate haze and improve visual predictability, thereby refining understanding of safety and efficacy in contemporary high myopia correction.
The analysis revealed no statistically significant difference between the two procedures in preoperative SE or SE at 1 month. These findings align with previous meta-analyses [10, 26]. At the 6-month postoperative mark, our meta-analysis revealed no significant difference in SE between PRK and LASIK initially; however, after excluding Zhang J. 2020, a statistically significant difference emerged in favor of PRK (MD: –0.29 D; 95% CI: –0.45 to –0.14; P = 0.0003). This suggests a potential advantage of PRK in refractive stability in the medium term. Curcă et al. also demonstrated significantly better SE outcomes at 6 months for PRK compared to LASIK, supporting this finding [28]. This difference reflects variations in corneal wound healing and biomechanical responses between surface ablation and flap-based procedures. In highly myopic eyes, deeper stromal ablation may predispose LASIK-treated corneas to early refractive regression, whereas PRK, particularly with modern ablation profiles and adjunctive usage of MMC, may allow more uniform stromal remodeling and improved refractive stability over time [6, 8]. Likewise, Mounir et al. reported stable SE outcomes over 12 months in both t-PRK and Femto-LASIK for high myopia, with no significant difference between groups at 6 months (p > 0.05), though their reported mean SE values at this point also numerically favored PRK (−1.08 ± 0.92 D vs. −0.74 ± 0.48 D) [14]. These findings reinforce our observation that PRK may yield more stable refractive outcomes at 6 months in patients with high myopia. By 12 months, the outcomes between the two groups converged again, with no significant difference observed in SE. A previous randomized clinical trial in low myopia patients has shown no significant difference in SE between PRK and LASIK at 12 months postoperatively [29]. While these findings were observed in patients with milder refractive errors, our analysis suggests this trend extends to high myopia populations as well. Moreover, a 12-month PRK series found that high myopic corrections maintained mean spherical equivalent near emmetropia and ≥20/20 UDVA in the majority of eyes, with efficacy and safety indices similar to those observed with lower myopia [30, 31]. This suggests that modern PRK provides excellent efficacy and safety across a wide myopic spectrum. Longer-term cohorts and predictive factor analyses further indicate that PRK maintains good stability over at least 2 years, and that higher myopia can still achieve efficacy indices close to those of low myopia when patient selection and surgical planning are carefully optimized [32].
In our meta-analysis, no statistically significant difference was found between PRK and LASIK in achieving a UDVA of 20/20 or better, before or after sensitivity analysis. After excluding Zhang J. (2020), heterogeneity decreased from 48% to 30%, further supporting the reliability of comparable outcomes between the two procedures. These findings are consistent with previous reports, such as the Cochrane review by Shortt et al., which found no difference in achieving 20/20 vision between PRK and LASIK in myopic patients, though most included studies involved low-to-moderate myopia [26]. When evaluating the more inclusive threshold of 20/40 or better, our analysis demonstrated a statistically significant advantage for LASIK (OR = 0.52; 95% CI: 0.32–0.85; P = 0.009), indicating that LASIK-treated eyes were more likely to achieve functional uncorrected distance vision in the high myopia subgroup. This finding was robust, with no heterogeneity among studies (I2 = 0%). Supporting this, El Danasoury et al. reported faster visual recovery and earlier achievement of functional vision following LASIK, especially in patients with higher refractive errors [29]. While PRK and LASIK may provide similar final high-acuity outcomes, LASIK may offer earlier functional gains in UDVA in highly myopic eyes.
The findings of this study showed no significant difference in final UDVA (logMAR) between PRK and LASIK, as also demonstrated in several comparative studies. Miraftab et al. reported that at 12 months postoperatively, PRK achieved a mean UDVA of 0.05 ± 0.13 logMAR, while Femto-LASIK achieved 0.02 ± 0.06, indicating highly similar uncorrected visual acuity outcomes in high myopia [33]. Similarly, Curcă et al. observed no clinically relevant difference in postoperative UDVA logMAR at final follow-up between PRK and LASIK-treated eyes [28]. Although LASIK has historically been associated with faster early visual recovery, our analysis and supporting evidence indicate that both techniques offer equivalent uncorrected distance visual acuity in the long term.
The pooled analysis indicated that LASIK demonstrated superior predictability in achieving a postoperative SE within ±1.00 D, particularly after excluding high-risk studies such as Zhang J 2020 and Hjortdal 2005, where the odds significantly favored LASIK (OR = 0.52; 95% CI: 0.29–0.94; p = 0.03). This observation agrees with the Cochrane systematic review by Shortt et al., which found that in eyes with moderate to high myopia, LASIK had a higher likelihood of achieving within ±1.00 D compared to PRK, although the difference did not always reach statistical significance (OR 0.58; 95% CI: 0.31–1.06) [26]. Similarly, Mounir et al. reported a higher proportion of eyes within ±1.00 D at 12 months following Femto-LASIK (85.71%) compared to t-PRK (71.43%) in high myopic patients [14]. For the stricter ±0.50 D target, the evidence was less consistent. The Cochrane review revealed no significant difference between LASIK and PRK in achieving ±0.50 D accuracy across all degrees of myopia (OR = 0.94; 95% CI: 0.42–2.11), with substantial heterogeneity noted (I2 = 53.9%) [26]. The cohort analyzed by Kaushik et al. demonstrated superior refractive predictability with LASIK-based modalities compared to PRK. Specifically, the proportion of eyes achieving a post-operative spherical equivalent within ±0.50 D of the intended target was significantly higher following Contoura LASIK (97%) and wavefront-optimized LASIK (95%) than after PRK (90%). Furthermore, patients in both LASIK subcohorts experienced accelerated visual recovery [34]. These findings support the interpretation that while both procedures provide acceptable refractive accuracy, LASIK may offer a slight advantage in predictability.
Corneal haze was reported in 8 studies; however, most reports originated from studies that did not routinely use intraoperative MMC. Seven of the eleven included studies did not report MMC use, whereas four studies used MMC and generally reported lower rates of clinically significant haze. MMC is now widely applied in contemporary PRK to inhibit keratocyte proliferation and reduce haze formation. In contrast, LASIK is distinguished by flap-related complications, as indicated by findings from 3 studies [14, 20, 22]. While rare, such issues can affect vision quality and may necessitate additional surgical management [35, 36, 37]. Proper surgical technique and adherence to postoperative care are crucial in minimizing these risks [20, 22].
This meta-analysis provides valuable insights into the outcomes of PRK versus LASIK in patients with high myopia. While both procedures offer comparable visual acuity at final follow-up, LASIK demonstrates superior refractive predictability and accuracy. Therefore, LASIK is preferred in cases where precise refractive outcomes and faster visual recovery are desired. However, the distinct complications must be considered. LASIK is more often associated with flap-related complications, whereas PRK is linked to delayed epithelial healing and corneal haze. In clinical practice, the choice of procedure should be tailored to the patient's characteristics, preferences, and lifestyle.
This systematic review and meta-analysis have several limitations that should be acknowledged. First, heterogeneity within the PRK and LASIK groups, including variations in surface ablation techniques (conventional PRK, transepithelial PRK, and advanced surface laser ablation), flap creation methods (femtosecond versus microkeratome LASIK), and the inconsistent use of Mitomycin C, may have influenced pooled outcomes and could not be fully explored through formal subgroup analyses because of limited reporting and sample size. Second, although several included studies were non-randomized and demonstrated moderate risk of bias, restricting inclusion exclusively to randomized controlled trials would have substantially limited the available evidence specific to high myopia. Given the relative scarcity of RCTs focusing solely on ≥ –6.00 D, the inclusion of well-conducted observational studies was necessary to provide a comprehensive assessment of this subgroup. Importantly, sensitivity analyses excluding higher risk and influential studies reduced heterogeneity and did not materially alter the direction or magnitude of the pooled outcomes, supporting the robustness of the conclusions despite methodological variability. Finally, publication bias could not be formally assessed using funnel plots due to the limited number of studies per outcome, and the findings should therefore be interpreted with appropriate caution. There are several key strengths to this study. A comprehensive risk of bias assessment was conducted to ensure transparency in evaluating the reliability of the included studies. The review focused on clinically relevant outcomes, including UDVA, refractive predictability, and postoperative complications, making the findings directly applicable to clinical decision-making. Furthermore, the systematic use of sensitivity analyses to address heterogeneity and assess the influence of outlier studies enhances the reliability of the conclusions.
Future myopic refractive research should prioritize large-scale, prospective, randomized controlled trials with extended follow-up durations. This prolonged tracking is vital for evaluating long-term refractive stability alongside the true incidence of late-stage complications, including corneal ectasia, regression, and chronic dry eye syndrome.
CONCLUSION
This systematic review and meta-analysis found that both PRK and LASIK are effective and safe options for correcting high myopia, yielding comparable long-term visual acuity and spherical equivalent outcomes. However, LASIK demonstrated superior refractive predictability, with a significantly higher proportion of eyes achieving ±0.50 D and ±1.00 D of the target refraction, as well as better odds of reaching 20/40 vision or better. PRK, while effective, was more frequently associated with postoperative haze and healing-related complications, suggesting that individualized procedure selection remains essential based on corneal profile and patient-specific risk factors.
Future studies should prioritize large-scale, prospective randomized controlled trials with extended follow-up beyond 12 months to assess long-term refractive stability and late-onset complications such as ectasia or regression. More consistent reporting of complications and standardized outcome measures across studies is needed to improve data comparability. Investigating newer surface ablation techniques (e.g., transepithelial PRK) and their performance in high myopia could further inform surgical decision-making.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: M.N.A.: Data analysis, statistical analysis, manuscript editing, and manuscript review. M.A.: Data acquisition and manuscript editing; G.A.: Data acquisition and manuscript editing; N.A.: Data acquisition and manuscript editing; A.A.: Manuscript editing and review; M.T.: Concept, design, definition of intellectual content, and manuscript review. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| CDVA | = Corrected Distance Visual Acuity |
| CI | = Confidence Interval |
| LASIK | = Laser-Assisted In Situ Keratomileusis |
| MMC | = Mitomycin-C |
| MD | = Mean Difference |
| OR | = Odds Ratio |
| PRK | = Photorefractive Keratectomy |
| RCT | = Randomized Controlled Trial |
| ROBINS-I | = Risk Of Bias In Non-randomized Studies of Interventions |
| RoB 2 | = Risk of Bias 2 |
| SE | = Spherical Equivalent |
| UDVA | = Uncorrected Distance Visual Acuity |
AVAILABILITY OF DATA AND MATERIALS
All data generated or analyzed during this study are included in this published article.
ACKNOWLEDGEMENTS
Declared none.